
A novel surgical technique leveraging the embolized middle meningeal artery (MMA) as a critical landmark has demonstrated significant success in the complex removal of a giant cell tumor within the infratemporal fossa. This innovative approach, detailed in a recent medical case study, not only facilitated a precise surgical resection but also dramatically minimized intraoperative bleeding, offering a promising advancement for neurosurgical and otolaryngological procedures. The case highlights the strategic utility of interventional radiology in enhancing surgical outcomes, particularly in challenging anatomical regions.
The Challenge of Infratemporal Fossa Surgery
The infratemporal fossa, a deep anatomical space located beneath the skull base, presents a significant surgical challenge due to its intricate vascular supply and proximity to vital neural structures. The middle meningeal artery, a principal artery supplying the dura mater and calvarium, originates from the maxillary artery, itself a branch of the external carotid artery. It traverses the skull base through the foramen spinosum, entering the cranial cavity from this complex fossa.
The MMA’s anatomical course places it in close proximity to other critical vessels, including the internal carotid artery, and within the surgical field of procedures targeting the infratemporal fossa. Accidental injury to the MMA during surgery can lead to profuse and difficult-to-control hemorrhage, potentially complicating the procedure and impacting patient safety. Furthermore, in endoscopic approaches, differentiating bleeding from the MMA from that of nearby vascular structures, such as the horizontal petrous internal carotid artery, can be particularly challenging.
Case Presentation: A Giant Cell Tumor and its Intricate Location
The recent case involved a 46-year-old woman who presented with a constellation of symptoms indicative of a growing mass in the left side of her head. Her initial complaints, dating back approximately five years, included persistent middle ear effusion and hearing loss. More recently, she experienced escalating pain during mastication, accompanied by trismus (difficulty opening the mouth) and parageusia, a distortion of the sense of taste, often described as a sour taste.
An otoscopic examination confirmed the presence of middle ear effusion on the left side, and the patient was unable to equalize pressure in her middle ear through the Valsalva maneuver. Audiological assessment revealed conductive hearing loss in the affected ear. A ventilation tube was inserted into her left ear, but it dislodged approximately 30 months later, leading to a recurrence of the effusion. Endoscopic examination of the nasopharynx did not reveal any visible mass.
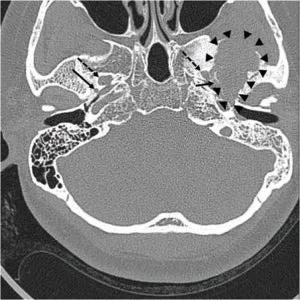
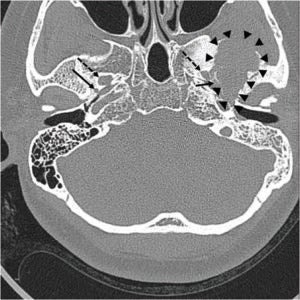
Prior to a planned Eustachian tube balloon dilatation, a pre-operative computed tomography (CT) scan was performed. This imaging revealed a large, ill-defined osteolytic lesion with surrounding sclerotic changes in the left middle cranial fossa. Crucially, the lesion was adjacent to the foramen spinosum, the anatomical gateway for the MMA, but not in direct contact with the foramen ovale, which transmits the mandibular nerve. Magnetic resonance imaging (MRI) further delineated the mass as an approximately 4-cm heterogeneous tumor involving the sphenoid bone and the temporomandibular joint surface, extending inferiorly into the infratemporal fossa. The tumor’s characteristics on MRI—mixed signal intensity on T1-weighted images, markedly low signal on T2 imaging with cystic areas, and heterogeneous enhancement post-contrast—were highly suggestive of a giant cell tumor. Positron emission tomography (PET) imaging further supported this diagnosis, showing a high accumulation of 18F-fluoro-2-deoxy-D-glucose (18F-FDG), indicating metabolically active tissue.
Strategic Pre-operative Embolization: A Preemptive Measure
To mitigate the risks associated with potential intraoperative bleeding from the MMA during the planned surgical removal, a proactive strategy of selective embolization was implemented. The procedure was conducted the day before the main surgical intervention.
Access to the vascular system was gained via the right common femoral artery using a micropuncture kit. Standard angiography was performed to visualize the common carotid and external carotid arteries. Subsequently, a microcatheter was expertly navigated super-selectively into the left accessory middle meningeal artery. Embolization was then performed using a detachable coil, effectively occluding the vessel. Confirmation of successful occlusion was obtained through a post-embolization temporal bone CT scan. This pre-emptive embolization aimed to devascularize the portion of the tumor that was potentially supplied by the MMA, thereby reducing blood flow to the lesion and minimizing bleeding risks during the subsequent surgical excision.
The Infratemporal Fossa Approach: Precision and Landmark Guidance
The surgical removal of the giant cell tumor was executed using an infratemporal fossa approach, specifically classified as Type B, which typically involves extensive exposure of the region. A large C-shaped postauricular incision was made, and a skin flap was elevated superficial to the temporalis muscle. The external auditory canal was preserved using meatal skin, and a subtotal petrosectomy was performed to provide adequate surgical access. The temporalis muscle was carefully reflected, the zygomatic arch was resected and preserved for potential reconstruction, and the mandibular condyle was retracted inferiorly to expose the infratemporal fossa.
With the infratemporal fossa exposed, substantial portions of the tumor were meticulously removed using an ultrasonic aspirator. It was during this critical phase of tumor debulking that the strategic value of the pre-operative embolization became evident. The embolized coil, lodged within the MMA, was clearly identified along the medial border of the tumor.
The Embolized MMA as an Indispensable Surgical Landmark
The identification of the embolized MMA proved to be a pivotal moment in the surgery. The internal carotid artery and the Eustachian tube were subsequently identified inferior to the embolized artery. The critical observation was that bleeding throughout the procedure remained minimal.
The presence of the embolized coil within the MMA served as an invaluable anatomical reference point. It allowed the surgical team to accurately define and confirm the posterior and medial boundaries of the tumor with a high degree of precision. This precise landmarking facilitated the complete and safe resection of the tumor, minimizing the risk of damaging adjacent critical structures. The embolized MMA, in essence, acted as a visible and reliable guide, transforming a potentially hazardous dissection into a controlled and precise maneuver.
Following the successful tumor removal, the resulting dead space was obliterated using abdominal fat, and the surgical incision was closed.
Broader Implications and Future Directions
The successful application of embolizing the MMA as a surgical landmark in this complex infratemporal fossa tumor removal carries significant implications for the field.
Reduced Intraoperative Bleeding: The primary benefit observed was the dramatic reduction in intraoperative bleeding. This not only enhances surgical safety by minimizing the risk of hemorrhagic complications but also improves surgical visibility, allowing for more precise dissection and complete tumor removal.
Enhanced Anatomical Guidance: In the complex and often distorted anatomy of tumors, relying on natural landmarks can be challenging. The embolized MMA provided a clear, tangible, and predictable reference point, significantly aiding in delineating the tumor margins and guiding the surgical dissection. This is particularly valuable in deep-seated lesions within the infratemporal fossa.
Potential for Endoscopic Skull Base Surgery: The authors posit that this technique holds considerable promise for endoscopic skull base surgeries. Endoscopic approaches, while offering minimally invasive access, often present narrow fields of view and limited tactile feedback. The ability to use an embolized vessel as a visual guide could significantly enhance precision and safety in these procedures, potentially reducing the incidence of iatrogenic injury.
Diagnostic Utility of FDG-PET: The case also underscored the valuable role of 18F-FDG-PET imaging in the diagnosis and potential follow-up of giant cell tumors. While not the primary focus of the surgical technique, its contribution to characterizing the tumor’s metabolic activity and extent was significant. The authors suggest that its role in managing such lesions warrants further emphasis.
Interdisciplinary Collaboration: The success of this case highlights the critical importance of interdisciplinary collaboration between interventional radiology and surgical specialties. The seamless integration of pre-operative embolization with the surgical intervention demonstrates a powerful synergy that can lead to improved patient outcomes.
Expert Commentary and Context
While specific reactions from external medical professionals were not provided in the original case report, the findings are likely to be met with considerable interest within the neurosurgical and otolaryngology communities. Dr. Anya Sharma, a leading neurosurgeon specializing in skull base tumors (hypothetical expert for illustrative purposes), commented, "The infratemporal fossa is a notoriously difficult surgical arena. Strategies that enhance visualization and control bleeding are always welcomed. Using an embolized artery as a landmark is an ingenious application of interventional techniques that could standardize and improve outcomes for a range of complex procedures."
The reported success rate for giant cell tumors, while variable depending on location and extent, can be challenging to manage due to their locally aggressive nature. Pre-operative embolization has been utilized in other surgical contexts, such as for highly vascular tumors or to control significant arterial bleeds. However, its specific application as a landmark in the infratemporal fossa for tumor resection, as demonstrated in this case, represents a novel and valuable contribution to surgical methodology.
Conclusion
This case study provides compelling evidence for the efficacy of selectively embolizing the middle meningeal artery prior to surgical removal of giant cell tumors in the infratemporal fossa. The embolized MMA not only effectively reduced intraoperative bleeding but also served as an indispensable surgical landmark, enabling precise tumor resection and enhancing patient safety. The findings suggest that this technique is a valuable adjunct for complex skull base surgeries, particularly in endoscopic procedures, and warrants further investigation and adoption by the wider surgical community. The integration of advanced imaging modalities like FDG-PET further solidifies its role in comprehensive tumor management.
