
Medical science has long grappled with the dual challenge of clinical efficacy and the complex nomenclature that defines its various disciplines. In the specialized field of otolaryngology—more commonly referred to as Ear, Nose, and Throat (ENT) medicine—the terminology often reflects a struggle to accurately categorize the vast array of conditions affecting the head and neck. While "oto" translates to the ear and "laryngo" to the throat, the term traditionally overlooks the complexities of the nasal passages, sinuses, and facial structures. Despite these linguistic hurdles, the history of medical terminology serves as a living record of human discovery, often drawing from mythology and historical figures to describe the triumphs and tragedies of the human condition. From the "Atlas" vertebra named for the Greek Titan to the harrowing "Ondine’s curse," which describes a fatal loss of involuntary breathing during sleep, medical names carry the weight of both lore and clinical observation.
Among these complex designations, Benign Paroxysmal Positional Vertigo (BPPV) stands as a quintessential example of a condition whose name is as unwieldy as its symptoms are disruptive. Often colloquially described as "loose crystals" in the ear, the clinical name is a precise, albeit lengthy, descriptor: it is "benign" because it is not life-threatening; "paroxysmal" due to its sudden, episodic nature; "positional" because it is triggered by specific head movements; and "vertigo" as it results in a false sensation of spinning. BPPV is not merely a medical curiosity; it is the most prevalent cause of vertigo worldwide. Clinical data suggests that approximately 9 percent of the elderly population suffers from undiagnosed BPPV, a statistic that carries significant public health implications. For older adults, the condition is a primary contributor to falls, which remain a leading cause of disability and accidental death in geriatric demographics.
The Biological Mechanism of the Inner Ear
To understand BPPV, one must first examine the intricate architecture of the human vestibular system. The inner ear utilizes dense calcium carbonate crystals, known as otoconia, within the otolith organs to sense gravity and linear acceleration. These crystals are essential for maintaining balance as they settle in response to movement. However, the system is susceptible to mechanical failure. When these otoconia become dislodged—due to aging, head trauma, or inflammatory disease—they can migrate into the semicircular canals, which are designed exclusively to sense rotational head movements.
Once these wayward crystals enter the fluid-filled semicircular canals, they transform a rotation-sensing system into one that erroneously responds to gravity. As the head moves, the crystals shift, dragging the endolymph fluid and creating currents that deflect the cupula—the sensory organ within the canal. The brain receives a high-intensity signal indicating rapid rotation, even when the individual is performing a simple task like lying down or rolling over in bed. This sensory mismatch between the vestibular signals and the visual input from the eyes results in the jarring sensation of vertigo and the accompanying nausea that characterizes the disorder.
While there are three semicircular canals, the posterior canal is the site of approximately 95 percent of BPPV cases. This is due to its anatomical "U-bend" shape, which acts as a gravity-dependent reservoir where debris naturally accumulates. Consequently, clinical specialists typically assume the posterior canal is the culprit unless diagnostic testing indicates otherwise.
A Chronology of Discovery and Medical Orthodoxy
The path to understanding and treating BPPV was marked by decades of trial, error, and institutional resistance. The first formal clinical description of the condition was published in 1921 by Robert Bárány, a Nobel Prize-winning otologist. Bárány’s career was as dramatic as his discoveries; a former student of Sigmund Freud—who allegedly rejected Bárány for being "too abnormal"—he served as a field surgeon for the Austro-Hungarian Empire during World War I. While held as a prisoner of war by Russian forces, Bárány received notification of his Nobel Prize, an honor that eventually facilitated his release through the intervention of the Swedish royal family.
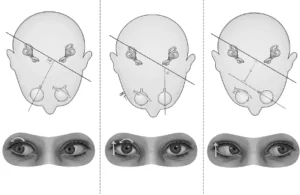
In his 1921 report, Bárány accurately detailed the "torsional" and "vertical" eye movements, known as nystagmus, associated with positional vertigo. However, like many of his contemporaries, he incorrectly attributed the cause to the otolith organs rather than the semicircular canals. This misconception persisted for decades, even as other researchers refined the diagnostic process.
In 1952, Charles Skinner Hallpike and Margaret Dix introduced the Dix-Hallpike maneuver, which remains the gold standard for BPPV diagnosis. Their research at Queen Square, London, focused on the "strange and dramatic" nature of the disorder. Despite their precision in identifying the "undermost" ear as the source of the symptoms, they too maintained the erroneous belief that the otolith organs were responsible for the dysfunction.
The field saw a significant shift in 1969 when Dr. Harold Schuknecht proposed the "cupulolithiasis" theory. By examining postmortem temporal bones, Schuknecht observed that certain parts of the inner ear degraded while the posterior canal remained intact. He deduced that crystals from the utricle had become embedded in the cupula of the posterior canal. While his theory was partially flawed—it failed to account for the specific direction of eye movements observed in patients—his status as the chief of the Massachusetts Eye and Ear Infirmary ensured that his ideas dominated vestibular science for years.
The Epley Revolution and the Fight for Acceptance
The modern era of BPPV treatment began in the early 1980s with Dr. John Epley, a practitioner in Portland, Oregon. Epley hypothesized that the crystals were not stuck to the cupula but were instead free-floating within the canal. He reasoned that a series of precise head maneuvers could use gravity to "guide" the crystals out of the canal and back into the vestibule where they belonged.
Despite the high success rate of his repositioning maneuver, Epley faced severe professional backlash. The American Journal of Otology rejected his initial submissions, citing that his findings were inconsistent with established medical theory. Throughout the 1980s, Epley was subjected to skepticism and formal investigations by medical boards. In one instance, an anesthesiologist filed a complaint against him, believing his maneuver was a sign of incompetence.
Parallel to Epley’s work, Dr. Alain Semont in Paris developed a similar repositioning technique. It was not until 1992—ten years after his initial discovery—that Epley’s work was finally published and recognized by the broader medical community. Today, the Epley and Semont maneuvers are celebrated as some of the most effective treatments in medicine, capable of curing a debilitating chronic condition in as little as two minutes.
Pathological Confirmation and Modern Clinical Data
The final confirmation of the "loose crystal" theory came through surgical observation. In 1990, Canadian surgeons Lorne Parnes and Joe McClure developed a technique to occlude the posterior canal for intractable cases of BPPV. During these procedures, they observed actual "debris" floating within the membranous tunnel of the ear. This material was later analyzed using scanning electron microscopy by Dr. Rick Chole and published in 2016, providing definitive visual proof of the wayward otoconia.
Further supporting data from researchers like Hui Xu has indicated that the source organ of these crystals—the utricle—often shows signs of dysfunction in BPPV patients, suggesting a systemic depletion of the crystal lattice. This evidence reinforces the understanding that BPPV is a mechanical failure of a biological system, rather than a neurological or inflammatory disease.
Broader Impact and Implications for Public Health
The resolution of the BPPV mystery represents a triumph of the scientific method over medical dogma. The implications of this discovery extend far beyond the treatment of "dizziness." By providing a rapid, non-invasive cure for the most common cause of vertigo, medical science has significantly reduced the risk of life-altering falls in the elderly.
Furthermore, the saga of BPPV serves as a cautionary tale regarding medical orthodoxy. The decades-long delay between the discovery of the cure and its widespread adoption highlights the need for the medical establishment to remain open to hypotheses that challenge existing paradigms. As the global population ages, the importance of vestibular health will only increase. While other conditions like Ménière’s disease remain without a definitive cure, the success story of BPPV provides a roadmap for future research: a combination of meticulous observation, anatomical understanding, and the persistence of individual clinicians against the tide of established opinion.
The work of Jeffrey D. Sharon and his predecessors ensures that the "Great Balancing Act" of human movement is better understood today than ever before. As diagnostic tools and repositioning maneuvers become more refined, the goal of illuminating all the secrets of the inner ear moves closer to reality, promising a future where balance disorders are no longer a permanent "curse" but a manageable, and often curable, mechanical hitch.
