
Medical professionals often describe the journey through medical school as a dual challenge: mastering the intricate art of healing while simultaneously acquiring a massive, often cumbersome, specialized vocabulary. Within the field of otolaryngology—commonly known as Ear, Nose, and Throat (ENT) surgery—this linguistic complexity is particularly evident. While terms like "otolaryngology" are technically accurate, derived from the Greek "oto" for ear and "laryngo" for throat, they frequently fail to encompass the full breadth of the specialty, which includes the sinuses, face, neck, and oral cavity. Yet, beneath these clinical labels lies a rich tapestry of human history, mythology, and the persistent struggle to understand the mechanics of human balance.
Among the most prevalent yet misunderstood conditions within this field is Benign Paroxysmal Positional Vertigo (BPPV). Often colloquially dismissed as "loose crystals" in the ear, BPPV represents a significant public health concern, particularly among aging populations. Recent clinical data suggests that nearly 9 percent of older adults suffer from undiagnosed BPPV, a condition that significantly elevates the risk of falls—a leading cause of disability and mortality in the elderly. Understanding the trajectory of BPPV from a misunderstood "curse" to a treatable mechanical issue offers a window into the evolution of modern otoneurology.
The Etymology of Ailment and the History of Anatomy
Medical terminology frequently serves as a living museum of human culture. The naming of anatomical structures often pays homage to the heroes and victims of medical history, as well as the myths that once explained the inexplicable. For instance, the uppermost cervical vertebra is named the "atlas," a reference to the Titan of Greek mythology condemned to carry the celestial heavens on his shoulders. Similarly, "Ondine’s curse"—a rare and life-threatening condition where the autonomic drive to breathe is lost during sleep—draws its name from European folklore involving a water sprite’s fatal retribution.
In the context of vestibular disorders, names like "Fregoli delusion" or "Ménière’s disease" anchor clinical observations to specific historical figures. BPPV, while lacking a mythological namesake, is defined by its clinical characteristics: "benign" (not life-threatening), "paroxysmal" (occurring in sudden episodes), "positional" (triggered by specific head movements), and "vertigo" (the false sensation of spinning). Despite its unwieldy name, BPPV is widely recognized by specialists as the most frequent cause of vertigo worldwide.
Particle Physics of the Inner Ear: How Balance Fails
To understand BPPV, one must look at the "particle physics" of the inner ear. The human vestibular system relies on a delicate arrangement of sensory organs. The otolith organs—the utricle and the saccule—utilize dense calcium carbonate crystals known as otoconia to sense gravity and linear acceleration. These crystals are essential for spatial orientation; however, through aging, trauma, or inflammation, they can become unmoored from their crystalline fortress within the utricle.
Once detached, this microscopic "flotsam" wanders into the semicircular canals, which are designed exclusively to detect rotational head movements. When a person with BPPV changes their head position—such as rolling over in bed or looking up at a high shelf—these wayward crystals settle like silt, dragging the endolymph fluid with them. This movement creates a current that deflects the cupula, a sensory receptor within the canal.
The brain, receiving high-velocity signals from the vestibular nerve, is misled into believing the body is moving rapidly when it is actually stationary. This sensory mismatch between the eyes and the ears results in the intense spinning sensation of vertigo and the rapid, involuntary eye movements known as nystagmus. Because the posterior semicircular canal sits at the lowest point of the inner ear’s anatomy—acting much like a U-bend in household plumbing—it is the site of approximately 95 percent of all BPPV cases.
A Chronology of Discovery: From Bárány to Epley
The scientific understanding of BPPV did not emerge in a vacuum but through a century of trial, error, and professional conflict.
1915–1921: The Bárány Observations
Robert Bárány, a Nobel Prize-winning surgeon and a former student of Sigmund Freud, published the first known clinical report of BPPV in 1921. While serving as a prisoner of war in Russia, Bárány continued his research into the vestibular system. His description of a young woman experiencing "rotary nystagmus" upon lying on her side was remarkably accurate, though he incorrectly attributed the cause to the otolith organs rather than the semicircular canals.
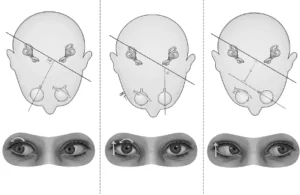
1952: The Dix-Hallpike Maneuver
Charles Skinner Hallpike and Margaret Dix, researchers at Queen Square in London, revolutionized the diagnosis of the disorder. They introduced the Dix-Hallpike maneuver, a diagnostic test that involves rapidly moving a patient from a seated to a supine position with the head turned. This maneuver remains the gold standard for diagnosing BPPV today. Like Bárány before them, however, Dix and Hallpike remained under the impression that the disorder originated in the otolith organs.
1969: The Cupulolithiasis Theory
Dr. Harold Schuknecht of the Massachusetts Eye and Ear Infirmary proposed the "cupulolithiasis" theory, suggesting that crystals became physically stuck to the cupula. While his theory was influential, it failed to explain why the vertigo episodes were typically brief, lasting less than a minute.
1980s: The Epley Breakthrough
The most significant turning point occurred in Portland, Oregon, where Dr. John Epley deduced that the crystals were not stuck but were "free-floating" within the canal—a theory known as canalithiasis. He developed a series of repositioning movements designed to use gravity to maneuver the crystals back into the utricle. Despite his success, Epley faced severe professional backlash. His work was rejected by major medical journals for years, and he was even investigated by the Oregon Board of Medical Examiners for "unprofessional conduct" due to his unorthodox methods.
Validation Through Modern Technology
The skepticism surrounding Epley’s "two-minute cure" was eventually dismantled by surgical and microscopic evidence. In 1990, Canadian surgeons Lorne Parnes and Joe McClure developed a procedure to occlude the posterior canal for intractable cases. During these surgeries, they observed physical "debris" floating within the canal, providing the first direct visual evidence of Epley’s theory.
In 2016, scanning electron microscopy conducted by researchers including Dr. Rick Chole finally confirmed the molecular makeup of this debris. The analysis proved beyond doubt that the particles were indeed wayward calcium carbonate crystals. Furthermore, studies by researchers like Hui Xu have demonstrated that in BPPV patients, the source organ (the utricle) often shows signs of dysfunction, suggesting a systemic depletion of the crystal lattice over time.
Clinical Implications and Public Health Impact
The implications of BPPV extend far beyond a simple "dizzy spell." In the geriatric population, balance disorders are a primary driver of institutionalization and loss of independence. Data from Dr. John Oghalai’s research indicates that the prevalence of BPPV is often underestimated because many patients attribute their instability to "old age" rather than a treatable mechanical issue.
The "two-minute cure"—the Epley maneuver—boasts a success rate often exceeding 80 percent after a single treatment. When compared to the long-term costs of fall-related injuries, including hip fractures and traumatic brain injuries, the rapid diagnosis and treatment of BPPV represent one of the most cost-effective interventions in modern medicine. Clinical observations show that once the crystals are repositioned, a patient’s fall risk typically returns to the baseline for their age group.
Broader Impact and the Future of Otoneurology
The history of BPPV serves as a cautionary tale regarding medical orthodoxy. The decade-long delay in the acceptance of the Epley maneuver highlights how established theories can sometimes obstruct the path to simpler, more effective treatments. Today, the Epley and Semont maneuvers are taught in medical schools worldwide, and physical therapists have become frontline providers in managing vestibular health.
As the global population ages, the demand for specialized balance centers is expected to rise. Future research is now shifting toward preventing the initial detachment of otoconia, looking into the roles of Vitamin D deficiency, osteoporosis, and vascular health in maintaining the integrity of the inner ear. While conditions like Ménière’s disease remain elusive in terms of a definitive cure, the success story of BPPV provides a blueprint for how scientific persistence and mechanical insight can transform a debilitating "curse" into a manageable, and often curable, clinical reality.
The scientific process, though often slow and self-correcting, has successfully illuminated one of the ear’s most common secrets. As experts like Jeffrey D. Sharon suggest, the journey from mythology to microscopic analysis ensures that the "great balancing act" of human life can be maintained with precision and care.
