
A novel surgical technique utilizing embolization of the middle meningeal artery (MMA) has demonstrated significant promise in enhancing precision and minimizing bleeding during the removal of complex tumors in the infratemporal fossa. This approach, highlighted in a recent case study, involved the successful resection of a giant cell tumor from a 46-year-old woman’s infratemporal fossa, where the embolized MMA served as a critical anatomical guide. The findings suggest a potential paradigm shift in managing challenging cranial base pathologies, particularly in endoscopic skull base surgeries where visual fields are often restricted.
Background: The Critical Role of the Middle Meningeal Artery
The middle meningeal artery, a vital branch originating from the external carotid artery’s maxillary artery, plays a crucial role in the vascular supply of the skull. It navigates its way into the cranial cavity by passing through the foramen spinosum, emerging from the infratemporal fossa. This anatomical pathway places the MMA in close proximity to numerous critical structures within the skull base and infratemporal region. Its significant blood supply to the dura mater and calvarium means that any inadvertent injury during surgical interventions in this delicate area can lead to profuse and potentially life-threatening hemorrhage. Surgeons operating in the infratemporal fossa, whether through traditional open approaches or less invasive endoscopic techniques, must exercise extreme caution when encountering this artery. The risk is further compounded by its potential to be mistaken for the nearby internal carotid artery, a critical vessel for cerebral blood flow, due to their anatomical proximity.
Case Presentation: A Challenging Tumor and an Innovative Solution
The case involved a 46-year-old female patient who presented with a persistent left-sided middle ear effusion and progressive hearing loss. Over a five-year period, she experienced increasing pain during mastication, culminating in trismus, a condition characterized by difficulty opening the mouth. Additional symptoms included parageusia (distorted sense of taste) and a persistent sour taste. Initial otoscopic examinations revealed middle ear effusion, and her Eustachian tube function was compromised, as indicated by her inability to inflate the middle ear via the Valsalva maneuver. A conductive hearing loss was confirmed by pure tone audiometry.
A ventilation tube was initially inserted into her left ear, but this provided only temporary relief, with the effusion recurring after the tube dislodged 30 months later. Endoscopic examination of the nasopharynx did not reveal any obvious mass lesions, leading to a plan for Eustachian tube balloon dilatation. Prior to this planned procedure, a high-resolution computed tomography (CT) scan was ordered.
Diagnostic Imaging: Unveiling the Extent of the Lesion
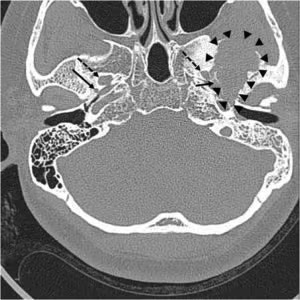
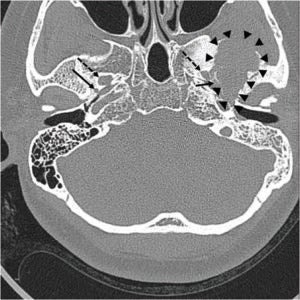
The pre-operative imaging played a pivotal role in diagnosing the underlying pathology and guiding the surgical strategy. The CT scan revealed a large, ill-defined osteolytic lesion within the left middle cranial fossa, accompanied by adjacent sclerotic changes. Crucially, the lesion was noted to be in close proximity to the foramen spinosum, the entry point of the MMA, but did not appear to involve the foramen ovale, which transmits the mandibular nerve.
Magnetic resonance imaging (MRI) further elucidated the nature and extent of the tumor. It confirmed that the lesion did not directly contact the foramen ovale but was adjacent to the foramen spinosum and the mandibular condyle. The MRI depicted an approximately 4-cm heterogeneous mass within the left temporal bone, extending into the sphenoid bone and the left temporomandibular joint surface. Notably, the tumor was observed to grow downwards into the infratemporal fossa. On pre-contrast T1-weighted images, the mass presented as a mixed iso- and low-signal lesion. T2 imaging revealed a markedly low signal within the tumor, with evidence of cystic changes. Post-contrast T1-weighted images showed a heterogeneous enhancement pattern, with intense enhancement of the cystic areas. These imaging characteristics were highly suggestive of a giant cell tumor, a type of bone tumor that can exhibit aggressive behavior.
Further diagnostic investigation involved a positron emission tomography (PET) scan. The PET scan revealed a strong signal indicating high accumulation of 18F-fluoro-2-deoxy-D-glucose (18F-FDG) within the infratemporal fossa, further corroborating the presence of an metabolically active and potentially aggressive tumor.
Surgical Intervention: A Pre-emptive Embolization Strategy
Given the size and location of the tumor, a surgical approach was deemed necessary. The chosen surgical technique was an infratemporal fossa approach, specifically Type B. A critical preparatory step was undertaken the day before the main surgical procedure: selective embolization of the left MMA.
This pre-emptive embolization was performed via a transfemoral carotid angiography. Access to the vascular system was gained through the right common femoral artery using a 5-French micropuncture kit. Standard 4-French diagnostic catheters were used to perform angiography of the common carotid and external carotid arteries. Subsequently, a microcatheter (Excelsior SL-10) and microwire (Synchro-14) were advanced under fluoroscopic guidance to selectively catheterize the left accessory MMA. Once positioned, embolization was achieved using a detachable coil, effectively occluding the artery. A follow-up temporal bone CT scan confirmed the successful occlusion of the MMA.
The Infratemporal Fossa Approach and the Role of the Embolized Landmark
The surgical removal of the giant cell tumor commenced with a large C-shaped postauricular incision. The surgical flap was elevated, carefully preserving the temporalis muscle. The external auditory canal was closed using meatal skin, and a subtotal petrosectomy was performed to gain optimal access. The temporalis muscle was then reflected, and the zygomatic arch was removed and meticulously preserved for potential reconstruction. The mandibular condyle was subsequently retracted inferiorly, providing direct exposure to the infratemporal fossa.
Using an ultrasonic aspirator, a substantial portion of the tumor mass was meticulously removed. During this phase of the dissection, the embolized coil within the MMA became clearly identifiable, situated at the medial border of the tumor. This visual confirmation was invaluable. The internal carotid artery and the Eustachian tube were subsequently identified inferior to the embolized MMA.
A significant observation during the procedure was the remarkably minimal bleeding encountered. The presence of the embolized coil in the MMA served as an indispensable surgical landmark. It allowed the surgical team to precisely delineate and confirm the posterior medial boundary of the tumor. This anatomical reference point facilitated a more accurate and controlled dissection, minimizing the risk of inadvertent damage to adjacent critical structures and contributing to the overall success of the tumor resection.
Following the complete removal of the tumor, abdominal fat was utilized to obliterate the resultant dead space, ensuring optimal healing and preventing complications. The surgical incision was then closed in layers.
Outcomes and Implications: A New Frontier in Skull Base Surgery
The successful outcome of this case offers compelling evidence for the utility of pre-operative MMA embolization as a surgical adjunct in infratemporal fossa tumor removal. The primary benefits observed were the significant reduction in intraoperative bleeding and the enhanced precision afforded by the embolized MMA acting as a clear anatomical landmark.
The authors postulate that this technique holds considerable promise for endoscopic skull base surgeries. In these minimally invasive procedures, the field of vision is inherently limited. The ability to identify a reliable anatomical marker like an embolized MMA could dramatically improve surgical accuracy, reduce operative time, and further minimize the risk of complications in such confined surgical spaces.
Furthermore, the role of FDG-PET imaging in the diagnosis and follow-up of giant cell tumors, as demonstrated in this case, warrants further emphasis. While not traditionally highlighted as a primary diagnostic tool for these lesions, its ability to detect metabolic activity and delineate the extent of the tumor proved to be a valuable asset in the pre-operative planning and understanding of the disease.
The implications of this refined surgical approach extend beyond this specific case. As surgical techniques continue to evolve towards less invasive methods, precise anatomical guidance becomes paramount. The MMA, being a consistent anatomical structure in the infratemporal fossa, when intentionally rendered visible through embolization, provides a tangible and reliable reference point. This can empower surgeons to navigate complex anatomical landscapes with greater confidence, ultimately leading to improved patient outcomes. The ability to pre-emptively control potential bleeding from a high-flow vessel like the MMA before surgical manipulation further enhances the safety profile of these procedures.
This innovative application of interventional radiology in conjunction with advanced surgical techniques underscores the growing interdisciplinary nature of modern medicine. The collaboration between radiologists and surgeons in cases like this is crucial for pushing the boundaries of what is surgically possible and for developing safer, more effective treatment strategies for challenging pathologies. The case serves as a strong foundation for future research and clinical trials to further validate and refine this technique for a wider range of skull base pathologies.