
A novel surgical technique utilizing the embolized middle meningeal artery (MMA) as a critical landmark during the removal of a giant cell tumor in the infratemporal fossa has been successfully demonstrated, offering enhanced precision and reduced bleeding, according to a recent medical case report. This innovative approach, detailed in the latest findings, highlights the strategic importance of vascular embolization not only for hemostasis but also as a visual guide in complex neurosurgical procedures.
Background: The Challenging Infratemporal Fossa
The infratemporal fossa, a deep anatomical space located below the base of the skull and medial to the mandible, presents a significant surgical challenge. This region houses numerous vital neurovascular structures, including cranial nerves, major arteries, and veins, making any intervention demanding in terms of anatomical knowledge and technical skill. The middle meningeal artery (MMA), a principal branch of the external carotid artery’s maxillary artery, plays a crucial role in supplying blood to the dura mater and cranial vault. Its anatomical trajectory, entering the skull base via the foramen spinosum from within the infratemporal fossa, places it in close proximity to critical structures and often necessitates careful navigation during surgery.
Historically, surgeons operating in this complex anatomical area have grappled with the potential for profuse and difficult-to-control bleeding from the MMA. Accidental injury to this artery, particularly during endoscopic endonasal approaches or direct infratemporal fossa dissections, can lead to significant intraoperative hemorrhage. The challenge is compounded by its anatomical proximity to other major vessels, such as the horizontal petrous internal carotid artery, which can lead to misidentification and further complications. The need for precise localization and control of vascular structures in this confined space has long been a focus of neurosurgical innovation.
Case Presentation: A Giant Cell Tumor and Its Complexities
The presented case involved a 46-year-old female patient who initially sought medical attention for persistent middle ear effusion and hearing loss on the left side. Over a five-year period, her symptoms evolved to include worsening pain during mastication, trismus (difficulty opening the mouth), and parageusia (altered taste sensation). Initial interventions, including ventilation tube insertion for the middle ear effusion, proved temporarily effective but ultimately unsuccessful as the effusion recurred.
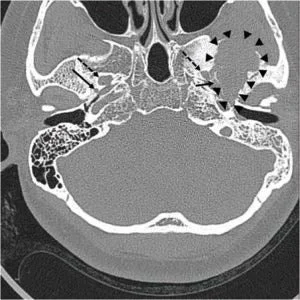
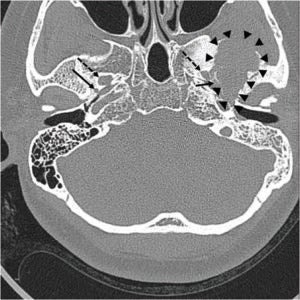
A pre-operative computed tomography (CT) scan, performed in preparation for planned Eustachian tube balloon dilatation, revealed an unexpected finding: a large, ill-defined osteolytic lesion with adjacent sclerotic changes in the left middle cranial fossa. Subsequent magnetic resonance imaging (MRI) provided a more detailed picture, identifying an approximately 4-cm heterogeneous mass. This tumor was located in the left temporal bone, involving the sphenoid bone and the left temporomandibular joint surface, with extension downwards into the infratemporal fossa. The MRI characteristics, including mixed signal intensities on T1-weighted images, markedly low signal on T2 imaging with cystic changes, and heterogeneous enhancement post-contrast, were highly suggestive of a giant cell tumor. Further investigation with positron emission tomography (PET) confirmed a strong uptake of 18F-fluoro-2-deoxy-D-glucose (18F-FDG), indicating metabolic activity consistent with a tumor in the infratemporal fossa. Crucially, imaging confirmed the tumor was adjacent to the foramen spinosum, the anatomical entry point for the MMA, but did not directly contact the foramen ovale.
Giant cell tumors are a rare group of bone tumors, characterized by the presence of multinucleated giant cells. While often benign, they can exhibit locally aggressive behavior and have a propensity for recurrence. Their location in the skull base and infratemporal fossa poses a significant surgical challenge due to the surrounding vital structures.
Strategic Intervention: Pre-operative Embolization
Recognizing the potential for intraoperative hemorrhage and the critical anatomical location of the MMA relative to the tumor, the surgical team opted for a strategic pre-operative embolization of the left MMA. This procedure was performed the day before the planned surgical tumor removal.
The embolization technique involved accessing the patient’s vascular system via the right common femoral artery using a 5-French micropuncture kit. Standard angiography was performed to visualize the common carotid and external carotid arteries. Subsequently, a microcatheter was advanced to selectively catheterize the left accessory MMA. Utilizing a detachable coil, the MMA was then occluded. Post-embolization temporal bone CT scans confirmed the successful occlusion of the artery.
This pre-operative embolization served a dual purpose: to reduce the blood supply to the tumor, potentially mitigating intraoperative bleeding, and to create a clearly identifiable vascular structure that could serve as a navigational aid during the subsequent surgical dissection.
Surgical Procedure: Infratemporal Fossa Approach
The surgical removal of the giant cell tumor was executed using an infratemporal fossa approach, specifically classified as Type B. This approach typically involves a postauricular incision, elevation of a flap, and reflection of the temporalis muscle. Key steps in this procedure include closure of the external auditory canal, subtotal petrosectomy, removal of the zygomatic arch, and downward retraction of the mandibular condyle to gain access to the infratemporal fossa.
During the extensive tumor debulking using an ultrasonic aspirator, the surgically embolized MMA became a prominent feature. The team identified the embolized coil within the MMA positioned at the medial border of the tumor. This visual confirmation of the embolized artery provided immediate anatomical orientation.
Enhanced Surgical Navigation and Outcomes
The presence of the embolized MMA proved invaluable during the surgical dissection. It clearly delineated the posterior medial boundary of the tumor. Inferior to the embolized MMA, the internal carotid artery and the Eustachian tube were identified, further reinforcing the anatomical landmarks. The surgical team reported that bleeding throughout the procedure remained minimal.
By using the coil within the MMA as a precise surgical marker, surgeons were able to accurately identify and confirm the tumor’s margins, facilitating a more controlled and complete resection. This navigational advantage is particularly crucial in the intricate anatomy of the infratemporal fossa, where distinguishing between tumor tissue and surrounding vital structures can be challenging. Following the tumor removal, abdominal fat was used to obliterate the created dead space, and the surgical site was closed.
Implications and Broader Impact
The successful application of this technique has several significant implications for neurosurgical and otolaryngological practices.
Reduced Hemorrhage: Embolization of the MMA prior to tumor removal directly addresses the risk of significant bleeding. By occluding this major blood supply, the overall vascularity of the operative field is reduced, leading to a safer and more manageable surgical environment. This is especially relevant in the context of tumors that may have neovascularization or a rich vascular supply.
Enhanced Precision and Navigation: The embolized MMA served as an invaluable anatomical landmark. In the confined and complex infratemporal fossa, clearly defined structures are paramount for accurate dissection. The visible coil within the artery provided a fixed point of reference, guiding the surgeons and minimizing the risk of inadvertent damage to adjacent structures. This is particularly beneficial in endoscopic skull base surgeries, where visualization can be limited by the narrow field of view. The embolized vessel acts as a tangible guide, enhancing the surgeon’s confidence and precision.
Potential in Endoscopic Skull Base Surgery: The report suggests that this embolization strategy could be highly beneficial in endoscopic skull base surgeries. These minimally invasive techniques rely heavily on precise navigation within confined spaces. Using an embolized vessel as a landmark could significantly improve safety and efficacy in these procedures, potentially reducing operative time and complications. The reduced bleeding and enhanced precision offered by this technique align perfectly with the goals of minimally invasive surgery.
Diagnostic Utility of FDG-PET: The case also highlights the underappreciated role of FDG-PET in the diagnosis and follow-up of giant cell tumors. While CT and MRI are standard for anatomical assessment, FDG-PET provides functional information about tumor metabolic activity. In this instance, the strong FDG uptake was crucial in confirming the diagnosis and could be invaluable for monitoring treatment response and detecting recurrence in future cases. The ability of FDG-PET to delineate active tumor tissue can aid in surgical planning and the assessment of post-operative residual disease.
Timeline of Events:
- Approximately Five Years Prior to Presentation: Patient begins experiencing pain during mastication.
- Recent Months/Years: Pain worsens, trismus develops. Patient also experiences persistent middle ear effusion and hearing loss.
- 30 Months Prior to Current Intervention: Ventilation tube inserted in left ear for middle ear effusion.
- 30 Months Later (Outpatient Follow-up): Ventilation tube dislodged, middle ear effusion recurs.
- Pre-operative Phase: Endoscopic nasopharyngeal examination negative for mass. Eustachian tube balloon dilatation planned. Pre-operative CT and MRI performed, revealing giant cell tumor. FDG-PET confirms tumor activity.
- Day Before Surgery: Selective embolization of the left middle meningeal artery (MMA) performed via transfemoral carotid angiography.
- Surgical Day: Infratemporal fossa approach Type B performed for tumor removal. Embolized MMA identified and utilized as a surgical landmark.
- Post-Surgery: Abdominal fat used for obliteration, wound closed. Patient recovers with minimal bleeding and precise tumor removal.
The findings from this case underscore the evolving landscape of surgical techniques in neurosurgery and head and neck surgery. The strategic use of pre-operative embolization, moving beyond purely therapeutic hemostasis to serve as an integral navigational tool, represents a significant advancement. As imaging modalities and interventional radiology techniques continue to improve, such integrated approaches are likely to become increasingly commonplace, offering improved outcomes for patients facing complex oncological and reconstructive challenges in critical anatomical regions. The successful application in this specific case provides a robust model for future surgical planning in similar challenging anatomical scenarios.